Atlas Monitor | 16 Oct 2021
[Atlas Monitor editor’s note: AM’s submission (with postscript edits/updates) to the COVID-19 Public Health Response Amendment Bill (No 2). Special thanks to Roger Bull and Voices For Freedom for their contributions]
Introduction
There is no justification whatsoever for either the original powers to be extended or additional powers added. Since the early days of the emergency measures in 2020 there has been a plethora of data which should have been incorporated into any measures used, especially when these measures take away fundamental freedoms.
This Bill’s measures move well past the minimum necessary to achieve public health aims and into the realm of totalitarianism. Many of the current and proposed measures are not proportionate, reasonable or necessary. They are not motivated by public health but rather a political agenda that fails to have the interests of New Zealanders at its core.
The Bill attacks the civil liberties of all New Zealanders. The control orders envisaged by the Bill run counter to a number of rights protected by the Bill of Rights Act. These rights are fundamental.
In particular – I object to all vaccine mandates. They are unethical and a gross infringement on the civil liberties and human rights of all New Zealanders. They are an obscene government abuse of power and tantamount to a pseudo-scientific dictatorship. There is no place in medicine for pressuring and coercing anyone into any medical intervention regardless of the perceived benefits.
As noted by Amanda Vickers, the deputy leader of the Social Credit party
Ethically, various codes have been designed to protect us from unconsented medical intervention. The Nuremberg Code set out to ensure no person had medical procedures performed without explicit consent. With the formation of the United Nations came the Universal Declaration of Human Rights as well as the International Covenant on Civil and Political Rights. New Zealand has a Bill of Rights (1990).
Mandatory vaccination entails the state appointing itself authority over the most sacrosanct – our bodily sovereignty. Doing so gives it the ability to deliver, to whom it wants, directly into our bodies, what it wants, in any amount it wants, whenever it wants.
Furthermore, the data simply neither supports nor justifies the mandating of vaccines. The morbidity and mortality profile of Covid-19 does not pose an overwhelming risk for the vast majority of people. Data from The United Kingdom and United States demonstrate that the risk of being infected with and dying from Covid-19 is very low. The risk is also stratified with huge variance between the very elderly and everyone else.
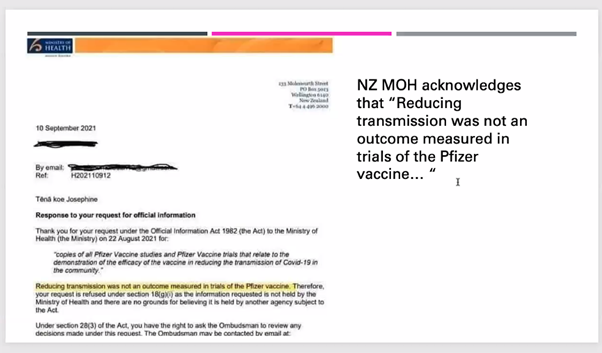
The absolute risk reduction conferred by the Pfizer vaccine does not support and mandate. Reducing transmission was not an outcome measured in the trials of the Pfizer vaccine. The vaccine does not reduce the viral load carried by infected people. Safety testing has been inadequate and the risk signals from the Covid-19 vaccine do not support any mandate. Pfizer’s conduct and in particular its history of fraud is a problem that seems to have been ignored.
Ultimately very few people are exposed to the absolute risk of Covid-19 infection but by attempting to vaccinate all of New Zealand the government is exposing the entire population to the risk of the well documented, albeit underreported, adverse effects of the Covid-19 vaccine. Promoting the benefits of vaccination over the risk and at the same time over-emphasizing the threat of the virus precludes informed consent.
New Zealand government officials claim that New Zealand’s pandemic response has been well executed and is following the data. They often point to overseas to argue what could happen when Covid-19 ostensibly gets out of control. An examination of the situation overseas is instructive.
The United Kingdom
The official UK government published case fatality rate for Covid-19 Delta variant for people under 50 years of age in the UK is 0.0%. This figure includes vaccinated and unvaccinated, people who are well and people with comorbidities. No massaging of the data. And this is the case fatality rate [the number of people who have died divided by the total number of people diagnosed with the disease], it is by definition higher than the crude mortality rate[the probability that any individual in the population will die from the disease].
Yes, that percentage again; 0.0%. Not a typo. Go to ‘Public Health England’, the official British Health Service information website. Look at SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 2’ table 4 on page 15. See below or this link.
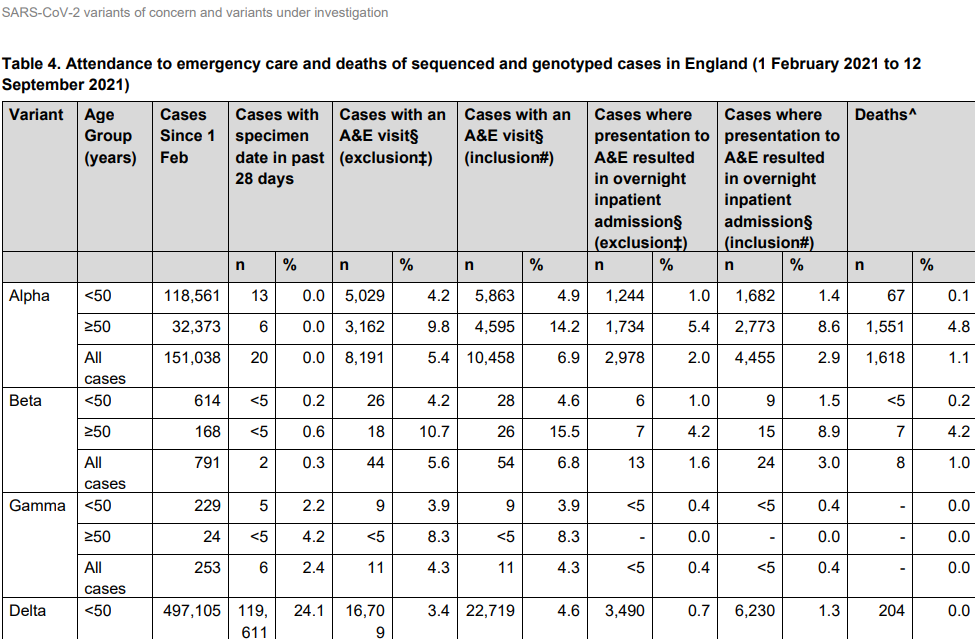
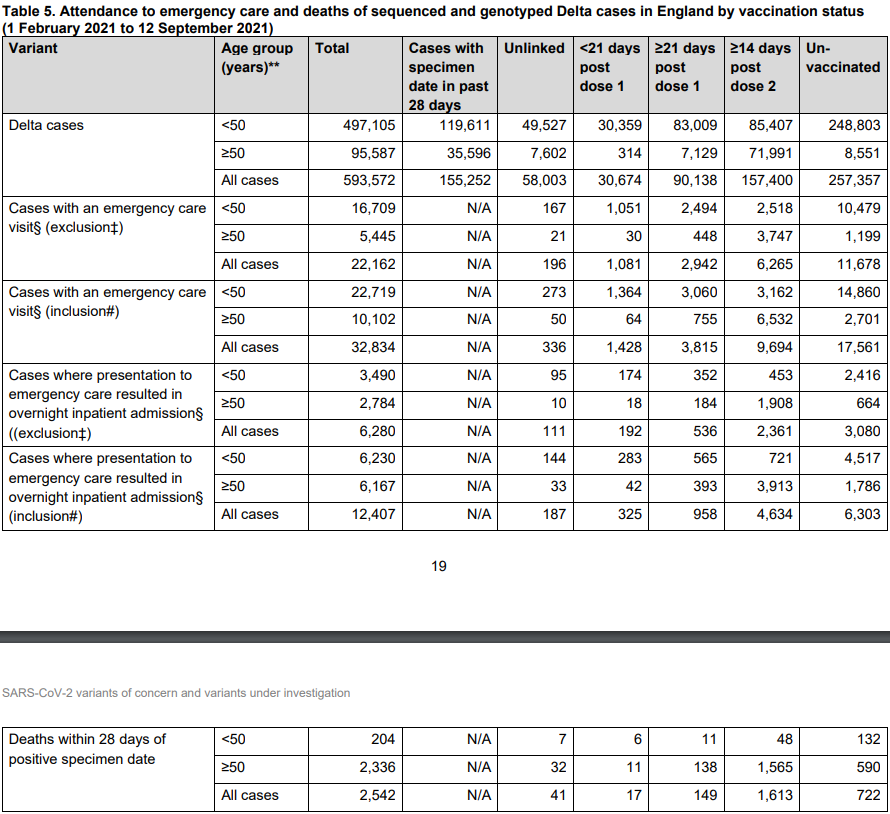
According to UK data[i] published 17 September 2021- 47% of new covid cases with the Delta variant were in the vaccinated. 43% were unvaccinated and the remainder unattributed to either vaccination status. 70% of deaths were vaccinated. 28% were unvaccinated and the remainder unattributed.
Prof Sir Andrew Pollard, Director of the Oxford Vaccine Group, said that vaccines did not stop the spread of Delta in the UK. This means that reaching the threshold for overall immunity in the population was “mythical.” Does anyone reading this doubt the Professor’s ability to accurately make this assertion? The UK Guardian found the spine to publish his words. Follow this link and see for yourself. Nor does the vaccine reduce viral load (the amount of virus in your body).
The United States
In the US the overall case fatality rate is 0.6%. Put another way, Americans have a 99.4% Covid-19 survival rate. Crude mortality rate is 0.2% [or 99.8% likelihood that you won’t die]. Americans have 1.86% chance of being hospitalised with Covid-19 [or 98.14% chance of not being hospitalised]. In other words, it’s overwhelmingly unlikely that one will get Covid19 and be hospitalised and die in the US. The CDC’s data shows that one in three Americans have tested positive for Coivd-19 and subsequently conferred natural immunity, then herd immunity is either close or has arrived.
The US seasonal flu has a case fatality rate of approximately 0.1% to 0.2%. Like Covid-19, this varies considerably across various demographics as noted by John Ioannidis [MD, DSc][ii], one of the most cited scientists in the world, who stated in his testimony to the US Senate that
the fatality rate from COVID-19 is highly dependent on age and modulated by the presence of comorbidities. For children and young adults, it appears that infection fatality rate is lower than seasonal influenza, and for middle-aged adults it is about the same. Infection fatality rate can increase sharply, however, when nursing homes are massively infected and when unprepared hospitals are overwhelmed and the infection spreads to hospitalized patients (nosocomial infection). This explains the paradox why COVID-19 is typically a very mild, benign infection, but it also has the potential to become devastating in specific settings.[iii]
Contrary to the perception that Covid-19 presents broad risk across the general population, it is in fact highly stratified with huge variance between young and old. According to Ioannidis age groups under 70 years old have survival rates well over 99%:
0-19: 99.9973%
20-29: 99.986%
30-39: 99.969%
40-49: 99.918%
50-59: 99.73%
60-69: 99.41%
70+: 97.6% (non-institutionalized)
70+: 94.5% (institutionalized and non-institutionalized)
A September 2021 US Department of Defense study[iv] looked at a cohort of 5.6 million Medicare beneficiaries all of whom were fully vaccinated. It revealed high rates of breakthrough infections of which 4% resulted in death. The study showed that 71% COVID-19 cases are breakthroughs in week after Delta variant > 90% and 60% hospitalized cases are breakthroughs in week after Delta variant > 90%.
This debunks the claim the Covid-19 is a pandemic of the unvaccinated. The data simply does not support this. Nor does it support booster shots because if the vaccine works then what problem are the booster shots supposed to solve? This was duly noted by British Medical Journal editor Peter Doshi during and FDA meeting[v].
Deaths misclassified as Covid-19 are an ongoing problem that is likely skewing data. Dying with and dying from Covid19 are often conflated. CDCs own data [table 3] states that in the US only 6% of these deaths, COVID-19 was the only cause mentioned on the death certificate. For deaths with conditions or causes in addition to COVID-19, on average, there were 4.0 additional conditions or causes per death.
Vaccines don’t stop spread of virus
A recent study in the European Journal of Epidemiology found that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people. This study looked at 68 countries and 2947 counties in the United States.
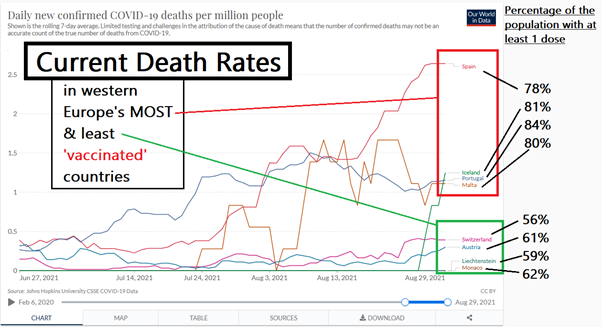
The official narrative that vaccination is synonymous with less virus is very difficult to believe, as the stated efficacy of all the Covid-19 vaccines to prevent transmission is not the actual efficacy [more on that to come]. This is clear from what is happening in Israel[vi], Iceland, the UK and other highly vaccinated countries.
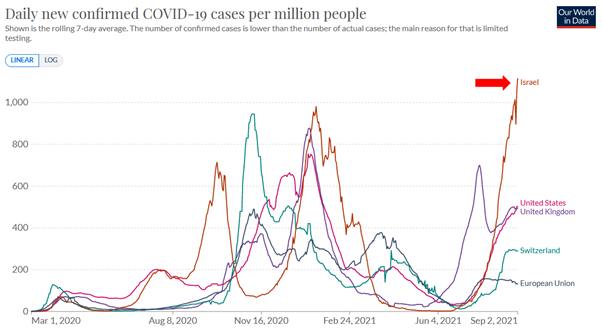
Israel, with an almost 80% vaccination rate of the eligible population over 12 years of age, has seen a massive surge in infection, hospitalisation and deaths. Israel is the best experiment in the world to determine what will happen to populations with very high vaccination rates. The majority of hospitalized Covid cases are fully vaccinated.
The reports, coming out of Israel, of adverse events following vaccination such as heart attacks and cardiac arrest in young people is a huge concern. Israel uses the Pfizer BioNTech vaccine and now claims it as just 39% effective.
A recent UK study by Imperial College London puts vaccine efficacy at stopping spread as 49% effective, not the claimed 95%.
Sweden and Portugal have banned fully vaccinated Israelis from entering the country. The Netherlands requires fully vaccinated Israelis entering the country to quarantine and produce a negative case. So much for this model vaccine rollout.
New Zealand
In New Zealand the case fatality rate is 0.68% and crude mortality rate is 0.0005%. As of 18 September 2021, there have been more than 20,000 reported adverse events from the vaccine in New Zealand, including 68 deaths reported post-vaccination. In the week ending 18 September there were 2,311 reported adverse events in total including 80 reported serious adverse events and eight deaths. 28 deaths with Covid-19 have been recorded in New Zealand total. More than twice as many deaths have been reported after vaccination than with or from Covid19.
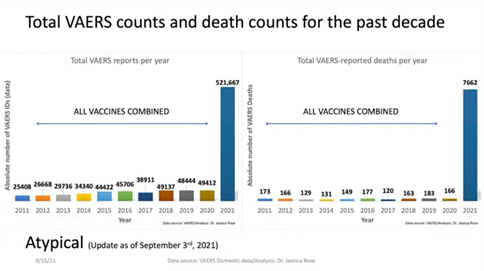
Let’s be clear. During the recent Delta outbreak in New Zealand, the first casualty was from the vaccine not the virus. That should not be surprising given the number of adverse events reported for Covid-19 vaccines to the Vaccine Adverse Events Reporting System [VAERS]. The number of reports of adverse events and death from Covid-19 vaccines exceed the reports of all previous vaccines combined from the last 20 years. This is a clear risk signal that is simply not being taken seriously enough.
Serious gaps in the data and undisclosed known risks
Pfizer have not provided data demonstrating that the vaccine does anything more than potentially relieve mild to moderate symptoms (i.e. the common cold) that could resolve on their own and have not provided data proving that the vaccine prevents or reduces infection and transmission, let alone hospitalisation and death. Pfizer New Zealand’s Sydney-based medical director Krishan Thiru admitted this on RNZ Morning Report. His comments begin at 07.47 in the interview. As the British Medical Journal points out, the trials simply have not been designed to prove any meaningful efficacy. An analysis in Forbes magazine shows that an examination of the vaccine study protocols reveals they are engineered to succeed. The article notes that
It appears that all the pharmaceutical companies assume that the vaccine will never prevent infection. Their criteria for approval are the difference in symptoms between an infected control group and an infected vaccine group. They do not measure the difference between infection and noninfection as a primary motivation … It boggles the mind and defies common sense that the National Institute of Health, the Center for Disease Control, the National Institute of Allergy and Infectious Disease, and the rest would consider the approval of a vaccine that would be distributed to hundreds of millions on such slender threads of success … It appears that these trials are intended to pass the lowest possible barrier of success.
Flawed safety testing and bias sample groups
In the safety testing that has been conducted the scientists eliminated all but the healthiest people in the sample group. If you smoked, vaped, had experienced any adverse reactions to vaccines previously, suffered allergic reactions to medication, had any psychiatric or any pre-existing conditions; you were excluded from the group. Pregnant women were also excluded despite being labelled a high-risk group. The exclusion criteria include ‘individuals currently working in occupations with high risk of exposure to SARS-CoV-2 (e.g. healthcare worker, emergency response personnel)’. These are the groups that the government is mobilising to mandate vaccination. It seems counterintuitive to exclude individuals from a Covid19 vaccine trial when they are the very people who are most likely to be exposed to Covid19 and therefore be vaccinated. Here are the full exclusion criteria.
The Pfizer trial is using the meningitis vaccine as a placebo in order to contrive a safety profile rather than ‘assist in blinding’ as claimed. If the studies consistently used an inert placebo, they would reveal far more adverse reactions from the Covid vaccine compared to the control [meningitis]. Both vaccines are acknowledged to cause tiredness (fatigue], fever and aches among other more serious side effects. They negate each other and so Pfizer can then claim that the vaccine produces no more adverse effects than the placebo and is therefore safe. This is disingenuous at best. Pfizer later offered the vaccine to the placebo cohort thereby eliminating the control group and precluding the harvesting of any data for long term safety studies.
Felony charges against Pfizer
Pfizer have been indicted on and plead guilty to felony violations in the US to the charges of fraudulent marketing of 13 different drugs. In 2009, Pfizer was ordered by US Department of Justice to pay US$2.3 billion in fines. At the time it was the
largest health care fraud settlement in the history of the Department of Justice, to resolve criminal and civil liability arising from the illegal promotion of certain pharmaceutical products.
Pfizer is a repeat offender. As noted in this article by The National Center for Biotechnology Information, part of the United States National Library of Medicine, it is abundantly evident that corporations such as Pfizer
treat both criminal and civil penalties as simply business expenses, to be weighed against the revenues earned from illegal behaviour … In the absence of such personal liability, both criminal and civil penalties appear to be, to Pfizer at least, a business expense worth incurring. You have to spend money to make money.
See Also:
- Pfizer to pay $2.3 billion, agrees to criminal plea
- “In the Army I was expected to protect people at all costs,” Kopchinski said in a statement. “At Pfizer I was expected to increase profits at all costs, even when sales meant endangering lives.”
- Nigeria sues Pfizer for $7bn over ‘illegal’ tests on children
- US Supreme Court rejects Pfizer Nigeria lawsuit appeal
- Pfizer in $486 million settlement of Celebrex, Bextra litigation
- Pfizer settles foreign bribery case with U.S. government
Pfizer intimidation and corporate liability immunity
Pfizer have also used bullying tactics on Latin American countries to secure vaccine delivery. The company is forcing countries to put up state assets as collateral to cover the potential cost of lawsuits stemming from adverse reactions after receiving the shots. In Argentina Pfizer went as far as asking ‘for additional indemnity from civil cases, meaning that the company would not be held liable for rare adverse effects or for its own acts of negligence, fraud or malice’.
The New Zealand government has granted Pfizer complete liability protection from any claims regarding adverse reactions to the vaccine. Specific details of the indemnity given to Pfizer, and other pharmaceutical companies supplying New Zealand with Covid-19 vaccines, are withheld under the Official Information Act (OIA). The Ministry of Health has taken the view that disclosure of such details ‘would be likely unreasonably to prejudice the position of the person who supplied or who is the subject of the information’. In other words, disclosure and any kind of detailed transparency might be a problem for Pfizer.
Pfizer’s misleading efficacy claims
Pfizer make claims of 95% efficacy with the vaccine. This is the relative risk reduction [RRR]. It is simply the difference in symptoms between vaccinated and unvaccinated trial participants. Out of the 18,198 people given the vaccine, 8 developed Covid19 compared to 162 of out 18,325 in the unvaccinated placebo group. This means that the risk of getting Covid19 if you’re unvaccinated is 0.88%. Vaccination reduces that risk from 0.88% to 0.04%. The absolute risk reduction [ARR] is therefore 0.84%, calculated by 0.88 minus 0.04. There is a 95% difference between 0.88 and 0.04, but that represents the RRR. Presenting the RRR in the absence of the ARR gives the impression that the risk reduction of the vaccine is better than it really is.
According to the journal Nephrology Dialysis Transplantation
relative risks do not tell us anything about the likelihood that the outcome would occur in each of these groups and how much higher or lower this risk is. To make sense out of a relative risk one needs to know the absolute risk that is simply the likelihood that an outcome will occur.
The point is that the risk of getting Covid19 is 0.88%, according to Pfizer’s data, if you are unvaccinated. That is less than one percent, which is very low by any measure. Getting vaccinated reduces that risk down to 0.84%.
Reducing transmission was not an outcome measured in the trials of the Pfizer vaccine
The vaccines were never designed to stop transmission so how can mandates be enforced as a public health measure, as it’s claimed, when they don’t stop transmission? They are personal treatment only. It is acknowledged that Covid19 vaccines do not block infection with SARS-CoV-2 and the New Zealand Ministry of Health states that ‘Reducing transmission was not an outcome measured in the trials of the Pfizer vaccine.’
To call these injections ‘vaccines’ is a misnomer. They do not prevent infection nor transmission. They do not confer immunity. They’re not a vaccine. They’re gene therapy products that turn your body into a viral protein making factory with no off-switch.
David Martin points out that that the primary end point of the Covid-19 vaccine trial is or at least ought to be prevention of symptomatic infection. However
The primary end point in the COVID-19 vaccine trials is not an actual vaccine trial end point because, again, vaccine trial end points have to do with immunity and transmission reduction. Neither of those was measured.
That is a profoundly poorly designed trial or scientific fraud. It calls into question the legitimacy of labelling these products “vaccines”. Vaccines are prophylactic i.e. they prevent illness. These products simply do not prevent disease. Presumably therefore, they do not meet the clinical definition of a vaccine and consequently the legal definition of a vaccine, unless of course the definition had changed.
The proclamation, that Covid is a pandemic of the unvaccinated is contradicted by the data. In a recent outbreak in Massachusetts, 3/4 of the people infected were fully vaccinated. Illinois recently experienced a cluster of “break-through” cases where 169 people died and 644 were hospitalized. Highly vaccinated Iceland recently had a spike in cases, the vast majority of whom were vaccinated.
We’re told that if we’re vaccinated we’re ‘less likely to die or be hospitalized’. That is simply not true and I’m sorry but to accept an irreversible procedure i.e. vaccination – I want some guarantees that are a bit more certain than “less likely” because “less likely” still happens. And it’s everywhere you look.
Dr. Sharon Alroy-Preis, Israel’s Director of Public Health and deputy CEO of the Carmel Medical Centre in Israel said, in a FDA advisory committee meeting[vii], that 60% of gravely ill (‘in severe and critical condition’) patients in her hospital were fully vaccinated and 45% who died in the fourth wave were also fully vaccinated.
It is also claimed that vaccine reduces symptomatic infection. However, data indicate that fully vaccinated people can carry as much Delta virus as unvaccinated people. There is an ominous implication here that the vaccine simply hides the symptoms and does nothing to reduce the viral load. This gives rise to the potential that asymptomatic vaccinated people with high viral load are spreading the virus unwittingly. This is signalled in the high vaccine uptake countries.
Children
Pfizer recently announced that it was seeking authorization from the FDA to vaccinate children 5 to 11 years old. As the New York Times noted
Pfizer’s clinical trial for children was not intended to draw meaningful conclusions about the vaccine’s ability to prevent disease or hospitalizations. Instead, researchers looked at antibody levels, comparing them with those that had conferred high protection in adults.
The trial involved just over 2000 children and is simply nowhere near large enough to be representative of the wider community and therefore cannot have any predictive value. A sample that small will not detect any risk of adverse effect. Given that children are at very low risk from infection and severe symptoms from Covid-19, safety should have been the main focus and priority. That does not seem to be the case. Incidentally adult trials involved up to 44,000 participants, which is still a relatively low number.
In a recently published study in the journal Toxicology Reports, the authors note that the majority of Covid-19 deaths occur in the elderly with high levels of co-morbidity; the number of children dying from Covid-19 is negligible; the trial samples are too small in numbers and too short in duration; and the trials do not address long-term effects most relevant to children.
In the UK, The Joint Committee on Vaccination and Immunisation [JCVI] has concluded that ‘the health benefits of universal vaccination in children and young people below the age of 18 years do not outweigh the potential risks.’
Conclusion
The Rule of Law is the fundamental cornerstone of any representative, constitutional democracy. It exists to protect the rights of all citizens. It does not exist to enable and facilitate a government policy agenda. Fundamental principles of the Rule of Law are being flouted by this government with this legislation, including that legislation should be consistent with the dignity of the individual and the presumption in favour of liberty.
Vaccine mandates contravene every principle of human rights and liberty. They are not supported by data and should not be enforced. Compelling people to take an experimental product that was rushed to market by a company with a demonstrable record of repeat offending and that has been afforded liability protection is very bad policy, let alone health policy.
Data from around the world shows that Covid-19’s morbidity and mortality profile does not pose enough of a threat for the vast majority of people, and in particular children, to justify vaccine mandates. The absolute risk reduction offered by the Pfizer vaccine is statistically insignificant. Countries with high vaccine coverage have not seen a reduction in infection and mortality. Indeed, there are safety signals from the vaccine that should be a cause for concern.
Too many real facts seem to have been missed by the government. Adhering to a dogma that results in an ineffective and potentially disastrous outcome will, in the fullness of time, be very difficult for those in power to explain. This point cannot be emphasized enough.
We are being told that vaccines and the vaccine passports are our tickets to freedom, but freedom cannot and should never be predicated on our medical choices. Medical intervention should always be a choice free from pressure, coercion as well as negative implications and consequences for those who decline vaccination.
What should be a medical decision has turned into a political dictate. This New Zealand government is seeking to remove our personal rights to bodily autonomy. It is simply unethical and it should stop immediately.
[i] Table 12, pp.19-20.
[ii] Professor of Medicine, of Epidemiology and Population Health, and (by courtesy) of Biomedical Data Science, and of Statistics and Co-Director, Meta-Research Innovation Center at Stanford (METRICS), Stanford University, Stanford, CA.
[iv] Salus Humetrix VE Study 2021-09-28a (1) https://www.scribd.com/document/530082359/Salus-Humetrix-VE-Study-2021-09-28a-1
[v] FDA Centre for Biologics Evaluation and Research (CBER) 167th Meeting of the VRBPAC, Public Comment Sep 17 2021 https://www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-september-17-2021-meeting-announcement
[vi] Israelis who were vaccinated were 13.06 times more likely to get infected after the shot than after natural infection https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.full.pdf
[vii] FDA Centre for Biologics Evaluation and Research (CBER) 167th Meeting of the VRBPAC, Public Comment Sep 17 2021

