Pierre Kory | 13 Mar 2022
The “narrative” that all positive ivermectin studies were small, low quality, fraudulent & could not be trusted was achieved via capture of the world’s leading ivermectin researcher, Dr. Andrew Hill.
My Global Disinformation Campaign Series:
Part I – Introduction to the Disinformation Playbook
Part II – Exposing the Corrupt Disinformation Campaign on Ivermectin
Part II – Ivermectin – An Attack by New York State’s Attorney General
Part III – Ivermectin – Lawyers Helping Doctors be Doctors
Part IV – Ivermectin – Saturday Night Fight At The Pharmacy
Part IV – Ivermectin – JAMA’s “Diversion”
Part VII – Op-Ed on Fluvoxamine
Part VIII – Op-Ed on Remdesivir
Part IX – “The Fix of Dr. Andrew Hill” – Chapter 1
Dr. Andrew Hill was hired by the organization UNITAID which was collaborating on the WHO’s ACT Accelerator program to research the efficacy of repurposed drugs against COVID. As a result, he became the world’s leading researcher on all the active and emerging randomized controlled trials of ivermectin in COVID since November of 2020.
Before I go into my personal and disturbing narrative of how “we” (Tess Lawrie and the FLCCC) discovered that Dr. Hill “got captured” and began to both allow and then openly attack the large body of supportive evidence of the efficacy of ivermectin, I want to take a moment to call attention to the recent work of a superb independent British journalist and documentary filmmaker named Phil Harper. His recently created Substack, called “The Digger,” tells the story in a more objective and deeply researched way, as he has uncovered details we suspected but did not fully know at the time this was all happening. He even managed to get Dr. Hill to meet him for a coffee interview in London recently. Wow. I also just did one of my best interviews yet on his podcast, (just kidding, that last link was to youtube and was predictably taken down within an hour of posting. New link on Rumble if interested. His questions and detailed knowledge of the subject matter allowed us to delve more deeply and powerfully into what is and was really going on. Anyway, please check him out, support his work with a paid subscription so he can devote more time to “digging” at the truth of this saga in an objective, fact-based, and highly skilled way (Pharma is not going to fund his work J). Also, I interviewed him on our FLCCC webinar this week to discuss his last post, which I think is one of the most major, historic, investigative “scoops,” in history, up there with the Watergate papers and numerous other scandals in the past decades.
Note this will probably be a three or more part post as it is and was the most damaging “tactic” of the global Disinformation campaign to distort and suppress the evidence of efficacy of ivermectin. Further, it is a post about events that “pre-date” this breaking story which is getting tons of attention. I hope to catch-up with all we have learned and are learning in the next few days.
Disinformation Tactic #5 from the “Disinformation Playbook” by The Union For Concerned Scientists.
THE FIX: Manipulate government officials, scientists, or processes to inappropriately influence policy
Before I explore what is arguably the most egregious example of “the fix” in terms of lives lost across the world, I must emphasize that the Disinformation campaign waged against ivermectin during 2021 was only the 2nd most damaging crime-against-humanity campaign against a generic, repurposed medicine in the pandemic. That first pandemic Disinformation Campaign targeted the life-saving COVID medicine hydroxychloroquine in 2020. Experts such as Dr. Harvey Risch and Dr. Peter McCullough and Dr. Richard Urso (among many others) had the front row seats to that one. They can likely tell equally dreadful tales of what they witnessed across media, medical journals, and societies/agencies, as that war, was, in some ways, way more sinister and depraved than the global war on ivermectin due simply to the fact that they used a tactic not possible against ivermectin; they literally created research studies using toxic doses of HCQ which ensured that the control group would survive at greater rates (fun fact: you can’t design such a trial with ivermectin because it is near impossible to make someone toxic from ivermectin (numerous propaganda media reports notwithstanding… and higher doses produce better results anyway). Paul Marik and myself are still reeling after reading the expertly detailed and highly referenced account of that disinformation campaign in Chapter 1 of RFK Jr’s book, “The Real Anthony Fauci.” Paul and I were both highly influenced by that campaign given we were “late” to understand its therapeutic efficacy (he more than me – despite Peter and Harvey telling us we were getting it wrong). I consider that book mandatory, assigned reading for all those being terrorized while living in a Pharma state. If I haven’t convinced you that we live in a Pharma state, then you must have missed the State of the Union Address that effectively served as a Pfizer commercial last week. Not subtle folks.
THE “FIX” OF DR. ANDREW HILL
I first met “Andy” soon after Senator Ron Johnson invited me to the Senate to give testimony in a hearing he was holding on early treatment on December 8, 2020, the video of which quickly went “viral” around the world (I must note that Senator Johnson, in my mind, stands out as one, if not the only, politician trying to fight back against the horrific suppression of early treatment and the abject failure of our agencies to control the pandemic). As a result of that testimony and the increasing attention to our comprehensive review paper on ivermectin that I had posted on a pre-print server a month before, I was invited to give the opening lecture at an international conference put together by the CEO of a French biotech company called MedinCell (they develop long-acting formulations of common medicines, allowing dosing to be as infrequently as every few months. Due to ivermectin’s protective efficacy against malaria, they were developing a long-acting formulation to be used in malaria prevention). They were also likely very interested in the potential application of ivermectin as a sort of “vaccine” against COVID (pretty cool huh?).
Anyway, the conference had about 12 lecturers from all over the world, from Dr. Kylie Wagstaff of the globally groundbreaking SARS-CoV2 cell culture study of ivermectin out of Monash University in Australia, to some of the principal investigators of the then ongoing or recently completed ivermectin RCT’s in COVID (even Prof. Elgazzar was there – he of the supposedly “fraudulent RCT”) to… a researcher sponsored by the organizations Unitaid and the WHO, a Dr. Andrew Hill.
He lectured on the 3rd day of the conference, (which I missed but Paul Marik did not). Paul watched every lecture of the three-day conference while I was busy battling to get our massive paper ready to submit for publication with a reference manager that was behaving so badly that I was literally having to reorder and re-number my references manually. All during this historic reference manager battle, new ivermectin studies and trials were getting posted on pre-print servers every day making me spend most of my days renumbering references. A Groundhog Day of epic proportions. Forgive me for I digress.
Anyway, Paul calls and asks, “Hey did you know that a guy from the WHO gave a lecture on his systematic review of all the randomized trials data on ivermectin in COVID?”
I was shocked. I thought our group was way ahead of everyone in our compilation of data (it turns out we were, more on that below).
I immediately wrote to the MedInCell CEO and asked for Dr. Hill’s slides and contact info. After receiving the slide deck, I was immediately blown away as it contained markedly positive RCT results.. that I was not even aware of. And he had done an actual data synthesis of the 11 RCT’s which was mind-blowingly positive in terms of reduced time to viral clearance, time to clinical recovery, need for hospitalization, … and death. At the time, those trials included about 1190 (or 890, I forget) total patients (note Paxlovid and Remdesivir got Emergency Use Authorizations based on less patients from single trials, the old “one and done” at the FDA). Andy responded immediately, we had an incredibly positive conversation, as any two researchers would when they think they may have stumbled upon data that potentially has global, historic impact. We started sharing our “origin stories” of how we had “discovered” the phenomenal efficacy of ivermectin in COVID.
Two critical pieces of information that I learned from that first conversation with Andy were;
1) His project scope specifically excluded looking at the RCT’s of ivermectin used in prevention. I cannot over-emphasize the catastrophic impacts of this. See below comment from the WHO guideline document and from the NIH document. They specifically avoid looking at ivermectin’s role in prevention despite at the time having results from 3 extremely well-done RCT’s with large magnitude benefits.. and this was before the massive Itajai study finding profound benefits when used as a preventive (which the agencies are nicely ignoring). Does it lie within the realm of possibilities that the reason may have been they were concerned about increasing vaccine hesitancy by identifying a super-safe, low cost, widely available alternative in prevention of COVID? Look at this crap from page 7 of the WHO guideline document from March 31st, 2021
Note that.. no reason is given for not looking at prevention. They just simply state that they will not look at prevention trials. Chilling.
From the NIH Guideline Panel document:

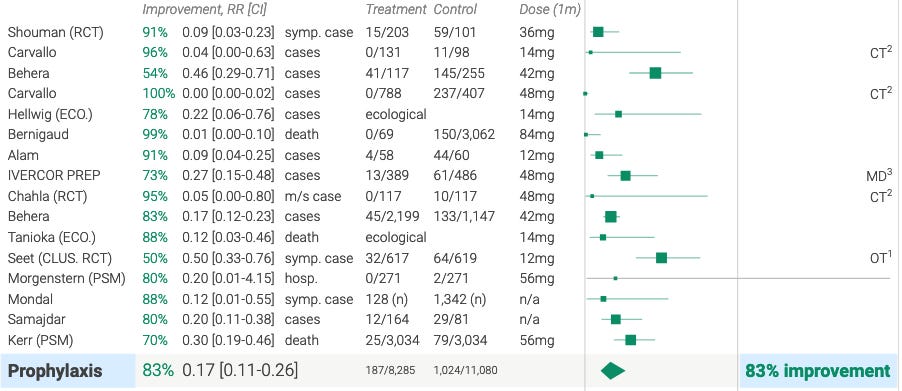
Note that although they mention trials in prevention, in their table 2D summary of IVM trials, only treatment RCT’s are included, and only a minority of them. Once again.. major health agencies are avoiding any look at or mention of the massive efficacy of ivermectin in prevention from trials starting in mid-2020. If you read my substack, you know how to interpret a Forest Plot. Here is the forest plot for prevention trials. Insanely protective, preventing 83% of infections.
2) His project scope specifically focused ONLY on RCT’s and no observational controlled trials. I cannot over-emphasize the catastrophic impact of this action, not only in this case, but in all of modern “evidence-based medicine” which I call “Big Science.” Over the past 2 decades, academic medicine now only believes in the results from “proper” trials which has been defined over the past years as large, prospective, multi-center, double blind RCT’s (PDBMCRCT) and this exclusionary over-reliance on such trials is essentially endorsed by nearly all the major professional societies and health care agencies. This belief has been influenced by the behaviors of “high impact medical journals” such as NEJM, JAMA, The Lancet etc. You just can’t publish trials that don’t fit this design in these journals, and any other trial design is automatically considered “low quality” evidence and is ignored. The reason why this is so injurious are many. I may expound more on this in a later in post, but briefly:
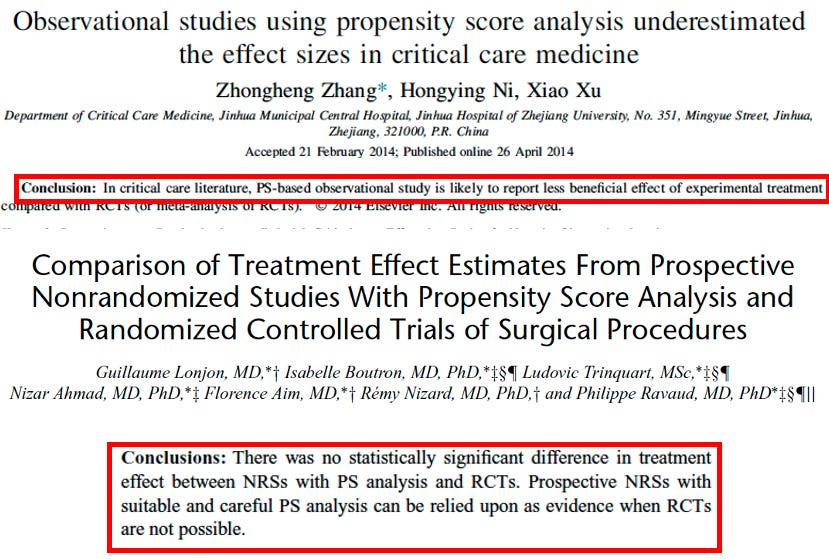
a. OCT’s and RCT’s, on average, over decades.. reach the same results – see this massive review comparing results from OCT’s and RCT’s from the Cochrane Library from a few years ago.
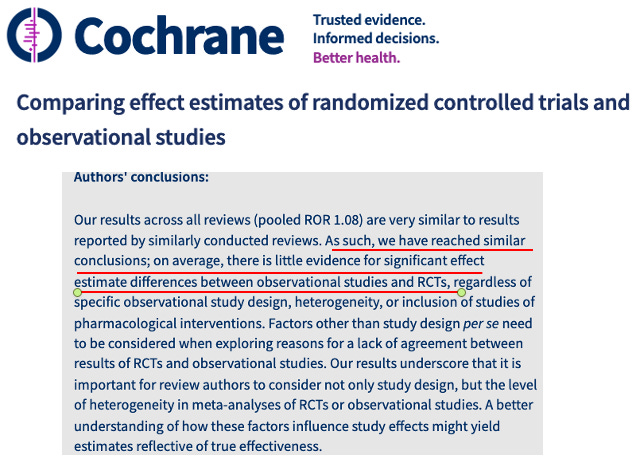
Note this was the “old” Cochrane Library, you know, the one before BMGF started giving it massive money, i.e. the “new” Cochrane library instead published an essentially fraudulent meta-analysis of just the RCT trials of ivermectin, using similar tactics to the WHO guideline (which I will get to very soon in Post 3 of this “series”) whereby they cherry-picked just 14 of the then available 24 RCT’s so as to find a supposedly “uncertain” efficacy. By the way, thinking about it a little more, can anyone explain to me why BMGF, purportedly an organization focused on public health and vaccinating the world.. gives so much money to major media organizations and to medical journals? Below slide from a recent lecture of mine.. contains just a handful of the media outlets getting money from him.

Did our Department of Health and Human Services (NIH, CDC, FDA), which Fauci effectively runs, take a page out of his playbook? This little bombshell came out this week:

I swear, every time I find a hit job from media or a medical journal, I can generally find BMGF as a major funding source within “two clicks” of the mouse. The insane retraction of our ivermectin review paper, after passing through 3 rounds of rigorous peer review by three senior scientists, occurred at “Frontiers in Pharmacology.” Two clicks and you get this:
Lets return to the catastrophic consequences of “Big Science” relying solely on just RCT data to guide medical practice:
b. RCT’s can be designed to fail (again, see the terrifying chapter on hydroxychloroquine in the book “The Real Anthony Fauci”). You wont be able to sleep after reading it. Just wait for Oxford’s Principle trial on Ivermectin (where they allow enrollees up to 14 days as outpatients) or NIH’s ACTIV 6 or U. of Minnesota’s trial where they gave only 3 days of therapy and allow up to 7 days to start treatment. Whatever.
c. RCT’s can be manipulated to produce over-inflated benefits by hiding inconvenient data (hello Pfizer vaccine trial and likely almost every other pharmaceutical company sponsored trial over decades).
d. PDBMCRCT’s can OFTEN fail to find mortality benefits even if well-designed without conflicts of interest, especially in diseases with heterogenous populations, heterogenous times to initiation of therapy, heterogenous outcomes, heterogenous care-centers, and heterogenous disease severity (the efficacy gets lost/diluted in such trials as it is not necessary in some, helps in others, and too late to make a difference in the moribund, thus statistically significant results are hard to find). In fact, in critical care medicine, not one has ever found a validated mortality benefit from such a trial prior to DEXA-ARDS in 2020. A thought leader in critical care even wrote an editorial calling for the abandonment of multi-center RCT’s in the ICU. Go figure.
e. If only PDBMCRCT’s move the needle, it should be noted that funding for such trials is only possible by big Pharma, NIH (same thing) and/or rarely, philanthropy – isn’t it interesting that the only as yet completed large PDBMCRCT’s of repurposed drugs were funded by “real” (not BMGF) philanthropists like the Rainwater Foundation and Steve Kirsch’s CETF.
i. A major reason why the exclusion of observational trials data is so damaging to science, is that well-meaning and committed clinicians and researchers (describes the majority of investigators that conducted Ivermectin trials in COVID) can do small “single-center” (a four letter word in academia) RCT’s or OCT’s easily and at low cost since OCT’s can be done via chart review comparing those who were treated with a medicine with those who were not. Many use a technique called “propensity score matching” to balance the comparison groups to approximate an RCT, and actually almost always reach the same conclusions and magnitude of effect as RCT’s. See below snapshots of slides from a talk I used to give when I was teaching (I mean, allowed to teach).
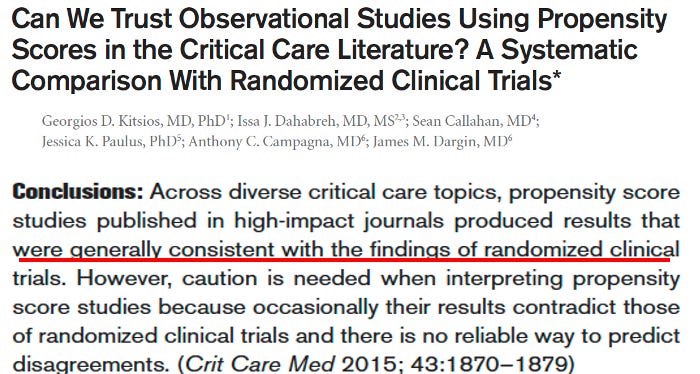
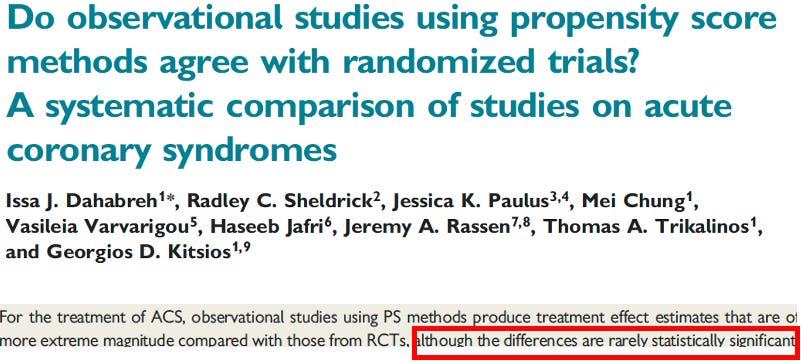
Imagine a world where your average doctor/researcher could do good research and find efficacy for something (god forbid a repurposed drug) and get it published in a big journal? Pharma would no longer control what can be studied in clinical trials, what trial results are allowed to appear in their medical journals, and thus what is allowed to be deemed “proven effective.” They would lose control of “the game.” Big Science. Please understand that there are decades of drug development with thousands of compounds and a million mechanisms of action. If serious and voluminous research into already available, repurposed, generic drugs were a central policy and practice of the NIH.. the entire business model and business of the bloated pharmaceutical industry would be decimated. If OCT’s were considered “legit” (which they most certainly are) therapeutic chaos for Pharma would ensue with many dozens of studies finding efficacy across many disease models of repurposed generic drugs, or gasp!.. vitamins and natural remedies.
Instead, trials of this design and focus do not get published in “big journals” and are instead dismissed as “low quality” and “insufficient evidence” and are ignored by the PHA’s (public health agencies) and academic societies. One startling exception in COVID was when Dr. Jean-Jaques Rajter in Miami, after 4 months of fighting with their reviewers and statisticians, was able to publish his propensity score matched study of ivermectin in hospitalized patients in the major American medical journal Chest. A wickedly positive study. Pharma must have missed that one, or pulmonologists stood tall. Who knows, but it “got through” the wall. Conversely, I cannot tell you how many study investigators have written to me telling me of the treatment they have recieved from journals for their “positive” ivermectin studies, typically met with rejection, or worse, “the hold”, where the journal holds the paper without sending it out for peer review.. and then rejects it two months later, depriving the world of critical information. Ask Professor Hector Carvallo, Professor Eli Schwartz, and Professor Flavio Cadegiani – happened to all of them. And not only them. Never mind, I will do a post about everything I know around the journals behavior of rejections..and retractions (what happened to many positive studies that “got through” peer review and were published only to be retracted).
iii. What a racket eh? Someday soon, I will tell the horror story of what the big journals and their RCT’s did to the role of intravenous vitamin C in severe sepsis (the topic over which Paul Marik and I became colleagues and close friends some years ago).
OK folks, since I digressed so much into Big Science, I am going to stop here for now, and Chapter 2 of “The Fix of Andy Hill” will follow shortly, beginning with both mine and Andy’s “origin story” of how we both got to studying ivermectin. Given what I have learned from “The Digger”, I now find his origin story downright ominous in retrospect. Stay tuned.
P.S. I just want to say how much I appreciate all the subscribers to my substack, and especially the paid ones! Your support is so greatly appreciated. Thanks my friends.


