Joel Smalley | 9 May 2023
We have to be honest – we are not going to win this war. The media propaganda is too strong and the public is too feeble-minded.
However, unlike other wars, the history of this one will not be written by the victors. Future historians will have a trove of evidence that will easily contradict the dogmatic assertions of those on the side of the official narrative.
One of those troves will be the Public Inquiry. Again, I have very little confidence that the conclusion will be honest and evidence-based but at least the evidence will be recorded for those who aren’t tainted by the globalist funding or suckered by their “trusted” government agencies.
In a similar vein, those who honestly chronicle the evidence today will be remembered favourably, and deservedly so too given the amount of illegitimate abuse they have had to endure.
One such chronicler is my dear friend, Dr Clare Craig – Co-Chair HART group. Diagnostic pathologist, lover of data, digital pathology and AI – according to her Twitter profile. I have seen her 175-page witness statement for the Public Inquiry, supported by almost 700 references. It is this sort of effort that makes such evidence credible.
Here is a very small excerpt, tweeted by her today (N.B. the use of 💉 instead of “vaccine” because illegitimate censorship of counter-narrative evidence is still happening in mainstream media).

I have been very busy recently preparing a witness statement for the covid Public Inquiry. They asked me to share details of deaths in 15-19 year olds males associated with 💉 rollout so I had to explain the bigger picture regarding concerns with these 💉. I said this:
Feb 2020 Whitty
said:
Covid not deadly enough to fast-track vaccines, Chris Whitty advised ministers
Chief Medical Officer gave opinion in February 2020 after Dominic Cummings mentioned Israel was planning to inoculate population.
“The rate limiting steps are late clinical trials for safety & efficacy, & then manufacturing. For a disease with a low (for the sake of argument 1%) mortality, a vaccine has to be very safe so the safety studies can’t be shortcut. So important for the long run.”
The belief that vaccines were safe had led to a circular belief that vaccines required fewer safety checks than other novel therapies.
Novel vaccines take a decade or more to go through saefety checks. Flu vaccines don’t. These novel drugs were treated like flu vaccines for regulatory purposes.
Pharma skipped testing for genotoxicity, carcinotoxicity and even studies showing how much spike is produced, for how long and where in the body it reaches. They said these studies were “not considered necessary.”

The trial info sheet said:
“Due to the urgent need for a vaccine against Covid-19, with agreement from the MHRA, some of the tests usually required for a newly manufactured vaccine have been modified, in order to make the vaccine available more quickly for assessment.”
The regulators let the pharma companies get away with trashing the placebo group after ~2 months by giving them the novel products. This was despite us knowing that narcolepsy caused by Pandemrix vaccine took on avg 8 months to be diagnosed.
Norwegian study links flu vaccine to narcolepsy risk
The Norwegian Institute of Public Health has found an elevated risk of narcolepsy among children and young adults who were vaccinated against the swine flu seven years ago. Some who did not take the vaccine against the pandemic of 2009 also developed this severe sleeping disorder.

AZ issued a press release claiming 100% efficacy against hospitalisation and death after only 2 severe covid hospitalisations and one death in the placebo arm.
This claim was repeated widely and was believed.
The priority was to protect the old and vulnerable who accounted for 98% of covid deaths. There were going to be 15 million jabs to freedom.

However, the WHO started a campaign in August 2020 that “no-one is safe until everyone is safe.” This penetrated and 💉 started to be aimed at healthy and ever younger arms.
The manufacturers decided to use the WHOLE Chinese spike sequence rather than parts of it, or peptides, which have been shown to be safer for vaccine design.

Some manufacturers modified the spike so that it could not bind to the receptor and enter a cell. This might have reduced some harm but the spike was delivered into cells – spike was produced INSIDE the cells in the first place.
AZ did not modify the sequence. From Nov 2020 it was clear that parts of AZ spike could be shed outside of cells.

There was total regulatory failure in allowing these products to be given to anyone which was compounded by not withdrawing them promptly once evidence these issues were clinically relevant became clear.
The huge numbers of failings has been set out by Perseus Group in The Perseus Report.

To touch on a few points: Since 2005 there were concerns about the regulator
“losing sight of the need to protect and promote public health.”

The CEO claims the MHRA is now an “enabler” not a “watchdog.”
https://www.youtube-nocookie.com/embed/xUQfzTqPUm4?rel=0&autoplay=0&showinfo=0&enablejsapi=0
No human studies were carried out to see what happened to the synthetic modified RNA – no-one knows how long it takes to be removed from the body. There is evidence that in some it lasts between at least 28 days and 4 months in the blood.
The lipid nanoparticles that devlivers the modified synthetic mRNA is toxic. This mechanism was shelved in 2016 for conventional gene therapy because of the multiple doses needed.

It was claimed it could still be used in vaccine technology because that only requires one dose… The viral vector used for delivering the AstraZeneca DNA message was reported in 2007 to cause platelet activation, which can lead to blood clots.
The Pfizer and Moderna clinical trial data shows a higher rate of serious adverse reactions from vaccine (12.5 per 10,000) than any reduction in serious events from covid (2.3 and 6.4 per 10,000 for Pfizer and Moderna respectively).

The adverse reaction alarm system blared red from January 2021. It was claimed this was due to over reporting because more people were informed about the system. Over the same time period reports for other drugs did not rise.
The US VAERS reporting system has been forced to release its data which shows signals of harm for 770 conditions 2/3rds of which were a stronger signal than for myocarditis & pericarditis which were acknowledged as a genuine adverse event in mid 2021.
CDC Finally Released Its VAERS Safety Monitoring Analyses for COVID Vaccines via FOIA
4 months ago · 555 likes · 181 comments · Josh Guetzkow
The spike protein is the most toxic part of the virus. It damages lungs, vessel walls and causes clots.
The Spike
A growing number of scientists are sounding the alarm about the risks of both COVID and its cures.

Part of the sequence is identical to a region of a bacterial sequence that can bind directly to a particular type of white blood cells resulting in lethal cytokine storms.
This part of the sequence was heavily mutated in the Omicron variant making it less lethal. However, even the most recent injections contained the original Chinese spike sequence with this dangerous sequence.
It has been difficult to measure the adverse reactions from the vaccines for three separate reasons: some were uncommon, some were slow to emerge and the risk was not present in every batch of vaccine.
Rare side effects like the brain clots and myocarditis are easier to be sure about because the impact on total numbers of those rare conditions is large.
Potential adverse reactions like, say, heart attacks or strokes, are so common normally after a certain age, that it would be very difficult to prove a cause, even if it were real, on an individual level.
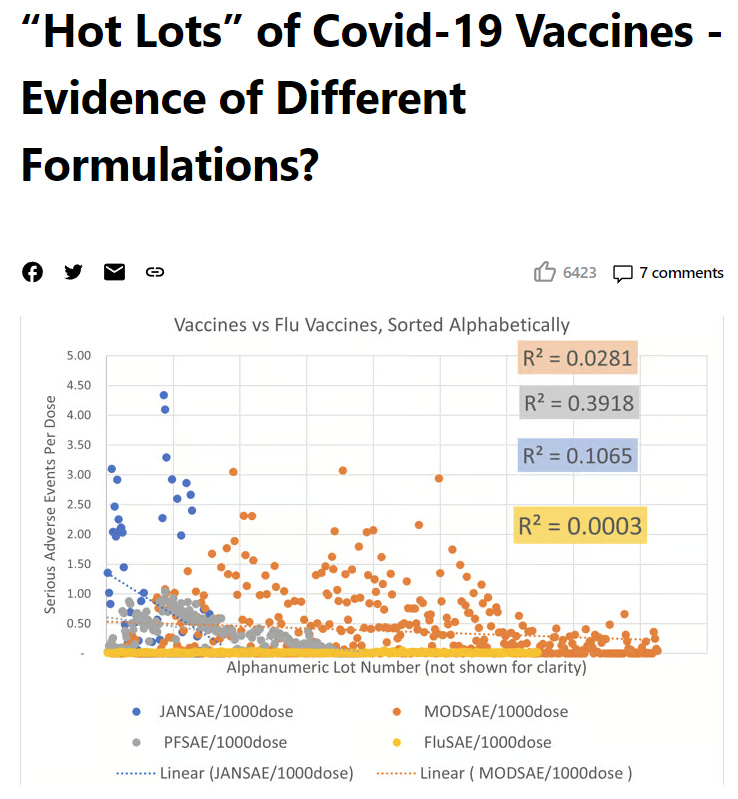
Certain batches of vaccine have had a much higher adverse reaction and death rate than others. A Danish study showed the rates of reports per dose fell into three categories of batch with high, medium or low adverse events.

One batch of Pfizer-BioNTech resulted in the hospitalisation of 120 children in Vietnam.

Those will include a small number of genuine coincidences. Reports filed by German doctors put the figure for serious reactions at 1 in 3,300 by September 2022.
Vaccine rollout coincided with a rise in pressures in hospital. Whereas covid had never resulted in a reduction in the number of empty hospital beds, once the vaccine rolled out there were increasing numbers of inpatients.

At the same time as there were reports of an accident and emergency crisis in the UK hospitals were overwhelmed in the USA.
Covid had never overwhelmed total hospital bed capacity anywhere.


All ambulance calls for life threatening conditions increased by 25 percent, an extra 500 calls every day from June 2021.

In late 2021, the vaccinated were attending the emergency department five times more frequently than the unvaccinated.

In Israel, there was a 25 percent rise in ambulance calls for cardiac arrests or coronary heart disease among 16 to 39 year olds. The rise was correlated to vaccination and not covid waves.
The Scottish data shows a clear rise in cardiac problems in the young.

It was claimed this was all due to the Delta wave or long covid effects.
But there is a control group.
Australia had had minimal covid and South Australia and Western Australia had had virtually none before Omicron.
Yet, their hospitals were also overwhelmed.In April 2022, Yvette D’ath Queensland health minister said she could not explain the rise in the most urgent ambulance calls (“code ones”).
Western Australia and South Australia had seen almost no covid before Omciron.
The graph shows total cumulative cases by state.

In Oct 2021, Mark McGowan, Premier of Western Australia said he could not explain the overwhelmed hospitals.
South Australia had fewer than 1,000 covid cases prior to December 2021. They saw 25,800 extra ambulance calls (mostly cardiac) from July 2020 to June 2021, which is about double the increase seen in the preceding two years.
The curious case of South Australian data
3 months ago · 56 likes · 42 comments · SADS
South Australia normally sees around 1,300 cardiac presentations per month for 15-44 year olds. This rose sharply in August 2021 with vaccine rollout, peaking at 2,172 in December. The whole state had seen only 1000 covid cases by 15th December.

Heart attacks can be caused by direct damage to the electrical circuitry of the heart, eg from inflammation or scarring because of myocarditis, or else can be due to slow narrowing of the vessel walls supplying the heart muscle due to inflammation.
A time lag should be expected.There was a notable rise in people who were not working because of long term sickness which began in spring 2021 when the vaccine was rolled out to the working aged population.

The rise was evident in males and females and also evident in the USA disability data.

In May 2022 the Governor of the Bank of England said there were 320,000 more people not working because they were sick.
At the time it was estimated from self reporting that only 80k had ever had symptoms of long covid.
There were 5 cases of cardiac or respiratory arrest in the group that received the Pfizer/BioNTech vaccine, compared to 2 in the placebo group.

If there was a small risk of increased death due to the vaccine in the period shortly after vaccination then this would be hard to detect in age groups where there were high numbers of background deaths.
However, in younger age groups, where there are fewer deaths normally, a signal might be noted.
This is what we saw for 15-19 year old males.
In females there was no signal.

Of the death reports in VAERS in 2021, there were 60% more males. This suggest these were not random but caused by spike induced pathology that also caused more males to die of covid.
Collapses and deaths on the football pitch saw a dramatic rise in the second half of 2021 that was ignored.

Players who were not playing because of “cardiac injury” also spiked doubling in number.

England saw a stepwise rise in cardiac deaths separate from covid waves.
These were deaths attributed to ischaemic heart disease deaths.

And these are deaths from heart failure.

It is harder to accurately predict expected deaths in winter periods which is heavily dependent on how many frail there are and which respiratory viruses are circulating. A quiet winter for deaths in the elderly in 2021/22 hid high deaths in the young and cardiac deaths.

Australia also so a rise in deaths before any significant covid.

It has just got worse since.

Some people have accepted that there were harms from these 💉 but then justify it in their minds saying they saved millions of lives.
The evidence does not support that position.
The claims are based on fantasy modelling.

It is true that the deaths per case fell with Delta but we have no influenza data to compare that to.
All we know is that for influenza each wave has a similar number of hospitalisations and deaths.
That is what we saw despite vaccination.

UK, Portgual and Ireland were outliers with a huge Jan 2021 spike and a more gradual Delta wave.
It is not good science to look only at the outliers.
It was Omicron that reduced mortality from Jan 2022.

We can further show this by looking at mortality in the first wave in places that did not have covid much before Omicron.
These places reached 500-600 deaths per million by Nov 2022.

That was the same order as Europe saw in the first wave.

As if that wasn’t bad enough, we now have evidence that the more doses given the higher the covid rates.

Chief Medical Officer of the UK


